As the debate about improving health in the United States wages on, it turns out that only 10 percent of our health status and longevity, experts declare, derives from health care.

DETERMINANTS OF HEALTH (1)
What Makes Us Sick?
As the Determinants of Health pie chart reveals, it is our behaviors, our habits (like excessive and poor eating, more than moderate drinking, smoking, physical inactivity, high salt and processed food intake), that drive the lion's share (40 percent!) of our ill health and early demise. It is also mental health conditions that often disable people and keep them from effectively managing their illnesses (2). While 30 percent of our health may be attributable to our genes, we now recognize through the science of epigenetics that genes are turned on or off by their exposure to our environment and what we do and don't do -- which helps to explain the rapidly growing rates of certain illnesses in this country.
Understanding the determinants of health is more than academic because of what it means to the quality of our lives and because the U.S. spends $2.7 trillion annually on health care services (18 percentof the GNP). Yet, this vast sum of money appears to influence only 10 percent of the health outcomes we achieve. Citizens of the U.S. may live longer than we did two decades ago, but we suffer from higher rates of morbidity (where functioning is limited by disease) and death when compared with 34 other developed nations (3). While we greatly outspend other countries for health care we have far too little health to show for it.
Of course, we want a top notch emergency room to go to if we have chest pain. We want skilled surgeons to operate on our vital organs and joints to sustain life, relieve pain and enhance mobility. We want (and need) scientifically proven disease management programs to slow the progression of the chronic diseases (like diabetes, heart disease, asthma, depression) that afflict our lives.
But it is population health, a growing movement in health policy and practices, that considers the wellbeing of a group of people and offers an approach that extends beyond the 10 percent of determinants managed by medical care delivered at hospitals, emergency rooms and even doctors' offices. Population health extends to the 90 percent of factors that make us sick.
What can be done?
Going beyond the pie chart of determinants of health leads us to the pyramid of factors that can improve our health.
This graphic, courtesy of the CDC and work by Dr. Thomas Frieden, depicts a graded approach of the actions a society can take to impact its health. But no level of the pyramid is meant to be primary or exclusive. The more levels affected the better we will mitigate disability and death.
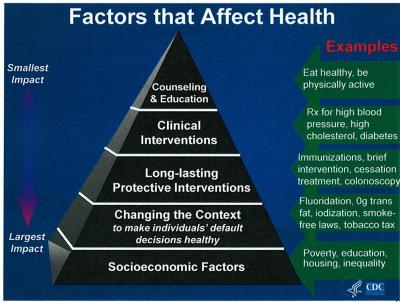
Achieving success on any level of intervention in the pyramid depends upon partnerships among public health proponents, medical centers, business entities, communities and citizens.
Stable and safe housing, even without health care, can stabilize chronic disease and reduce unnecessary emergency room and hospital care. Smoke-free environments can reduce respiratory illnesses and cancer. Early detection of cancer, colon and breast cancers for example, allows for earlier intervention and reduces death. Early detection in primary care or community settings of hypertension, diabetes, high cholesterol and depression improves lives and saves money. Self-care with diet, exercise and stress management are at the heart of healthy communities and nations.
Is Population Health Possible?
What makes us think that population health can be achieved? The natural act of self-interest may answer that question. We are far more apt to do something if it is shown to be in our self-interest or the interest of those we care about -- and when it is built into the routines of medical care and our lives.
We now have inescapable evidence that illness is bad for business. We know that illness produces absenteeism, presenteeism (showing up but being unproductive), and greater rates of disability. We also know that wellness ("... a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity." -- The World Health Organization) increases worker (from the factory floor to the corner office) productivity and is associated with higher corporate earnings (so says IBM).
We know that 1 percent of patients in a large group of people account for about 20 percent of medical costs; that 5 percent of patients account for 50 percent of costs; and that 10 percent of patients account for 75 percent of costs. But if only 10 percent of their health is determined by the provision of health care we are talking about a tiny fraction of what can reduce costs.
Enter population health: Unless we change behaviors and the environments people live and work in there will be limited impact on the economic burden a society and a community face. In other words, we can't afford to still primarily focus on medical care.
We also have a sea change underway in the financing of health care. Buyers of health care (federal and state governments and large employers in the private sector -- the vast predominance of the purchasers of medical services) are now putting in place payments that will reduce reimbursing medical providers for doing more and instead incentivize them to economically contain the health costs of their subscribers. When health plans and medical practices are put at financial risk for not managing to a fixed budget or, even better, create arrangements where savings are shared by purchasers and providers together, the marketplace can add its muscle to achieving health. Penalties like not paying for inpatient readmissions within 30 days also drive better health. They force hospitals to be partners with communities and with patients (and families) since what happens after a hospital stay usually has little to do with what happened in the hospital and everything to do with follow-up care and the attention patients give to their health.
Privacy concerns notwithstanding, we also are seeing an explosion in information technology -- the nervous system of health care. We are positioned to place a cortex, an IT cortex, to inform and help improve the health of patients and populations. Information need not stop at the grounds of a hospital. Patients, primary care clinicians and medical practices can (and are doing so in demonstrations underway) be linked to information about what consumers buy in the supermarket, the fitness they pursue with pedometers and in clubs, and their smoking and drinking habits. If Netflix and Amazon can know so much about you and influence what you buy and do, so can health IT. What's more, insurance premiums paid by subscribers may come to reward, or not, those whose habits are less costly to society. Using information to shape public behaviors may be called the "nanny state" but it is also a way by which individuals can take control of their health while businesses as well as state and municipal governments save money and lives.
Who is leading the way?
I recently attended a meeting, a Population Health Summit, in New York City, hosted by the NYS Department of Health with the support of the NYS Health Foundation, the NYC Department of Health and Mental Hygiene, hospital associations, NYS county governments, community health care providers, researchers, global and local companies, universities, and the NY Academy of Medicine. We met at the headquarters of the NY Academy of Sciences.
Attendees were there to advance the cause of population health: to assert the evidence for it and to provide examples of what can and is being done. The message throughout the day was that it is possible to reduce illness and death, improve quality of lives and "bend" the curve of (if not diminish) budget breaking health care costs by attending to more than the 10 percent that has dominated our health care heretofore.
To do so, however, requires unprecedented collaboration among the varied groups assembled -- who need proof that they can achieve results consistent with their respective interests. Hospitals have had to fill beds and do complex procedures to remain financially viable. Governments have had to regulate to try to control costs and quality. Businesses, large and small, have struggled with the growing burden of health insurance costs and have done what they need to do to limit them. Researchers have had little opportunity -- or support -- to move from controlled, university settings into the barrio, the supermarket aisle, domestic dysfunction and damaging human habit disorders.
Among the prominent public health experts at the Summit were Drs. Tom Frieden (head of the CDC), Nirav Shah (NYS Health Commissioner) and Tom Farley (NYC Health Commissioner). Their message to the diverse interests in attendance was that population health can be financially sustainable and can get NYS (and this country) out of the global cellar of rates of morbidity and mortality.
But experts, government officials and corporate buyers cannot succeed without individuals and families coming to believe that their interests will be served, their lives improved and their personal budgets spared by taking their health seriously. Changing habits is among the most daunting of endeavors for any of us. But we now have behavioral interventions like Motivational Interviewing (4) and Screening and Brief Intervention and Referral for Treatment -- SBIRT (5). We have smart phone apps (and other technologies) for monitoring and managing just about everything human from the food we ingest to the moods we have. Peer influences are helping to reduce smoking and excessive sugary drinks. Insurance incentives to live healthy can add leverage for prevention and self-care. No single intervention works here either but when bundled together people do change.
Population Health
Population health will not be achieved by a few missionaries. But it can be led by a confederation of public health advocates, organized medicine, government, independent businesses, and patients and families. What seems out of reach is possible when so many players are on the same team.
As individuals, we can benefit from new medicines and more frequent MRIs, surgery or other procedures. In fact, we have an amazing health care system in this country that does just that for those who have good medical insurance. We don't want to lose that capability; we want to add to health care the needed attention to the 90 percent of determinants that impact our health, our longevity and our pocketbooks.
To paraphrase President John F. Kennedy, changing the public's health will not be easy -- it will be hard. Those gathered at this Summit on Population Health were there for the sake of our generation and the generations to come. Let's wish them well and lend our collective support for they surely will need it.
References:
1. McGinnis, JM, Williams-Russo, P, Knickman, JR: The case for more active policy attention to health promotion. Health Affairs, 2002;21:78-93
2. Sederer, LI, Chung, H: The cost of not caring for people with serious mental illness, The Huffington Post, July 16, 2013, http://www.huffingtonpost.com/lloyd-i-sederer-md/mental-health-care_b_3605777.html
3. US Burden of Disease Collaborators. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors [published online July 10, 2013]. JAMA. doi:10.1001/jama.2013.13805
4. Miller WR, Rollnick S. Motivational interviewing: preparing people for change. 2nd ed. New York (NY): Guilford Press; 2002.
5. Bernstein, SL, D'Onofriodoi, G: A Promising Approach For Emergency Departments To Care For Patients With Substance Use And Behavioral Disorders, Health Affairs, 32, no.12 (2013):2122-2128 (10.1377/hlthaff.2013.0664)
---
Dr. Sederer's new book for families who have a member with a mental illness is The Family Guide to Mental Health Care (Foreword by Glenn Close).
The opinions expressed here are solely mine as a psychiatrist and public health advocate. I receive no support from any pharmaceutical or device company.