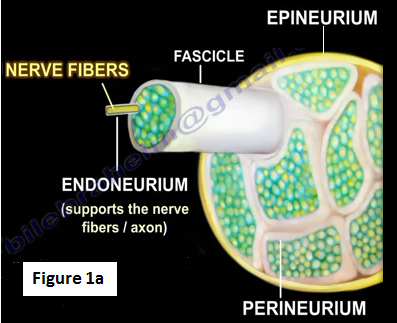
The anatomy and structure of any nerve is complex. A nerve is a bundle of axons that are grouped into fascicles. Nerves provide a pathway for impulses to be transmitted along each of the axons to the limbs and organs.
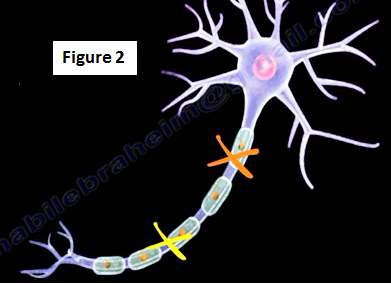
A cross section of the nerve is shown in figure 1a. The epineurium is a thick connective tissue layer that covers and protects the nerve. The perineurium is a sheath that covers the fascicles and the endoneurium surrounds each axon. The myelin sheath acts as insulation cover that protects the neuron. The myelin sheath also allows the signal to move faster along the axon (Figure 1b). Injury to the axon may be a single or double crush injury (Figure 2). Classification of the nerve injury depends on the nerve components affected, loss of functionality and the ability of the nerve to recover.

Two grading systems are used to define the extent of the nerve injury; Seddon's and Sunderland's. Seddon's classification includes neurapraxia, axonotmesis, and neurotmesis in the order of increasing severity. Sunderland's classification has five grades of nerve injury. Seddon's classification is the classification of nerve injuries that most physicians use. Nerve injury is classified by Seddon into three types: neurapraxia, axonotmesis, and neurotmesis.
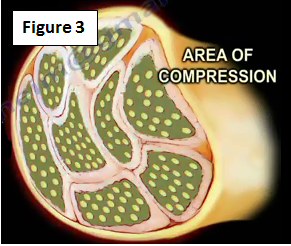
Neurapraxia (Figure 3)
The prognosis is good with neurapraxia and it's the mildest form of nerve injury and the nerve remains intact. This causes a temporary loss of motor and sensory function due to blockage of the nerve conduction. No conduction will occur across the area of injury. The injury may result from compression of the nerve or pressure ischemia. The signaling ability of the nerve is damaged; however, this injury usually recovers completely since there is no axonal injury. It may take up to 12 weeks to recover. There is no fibrillation; fibrillation is only seen when there is an axonal injury.
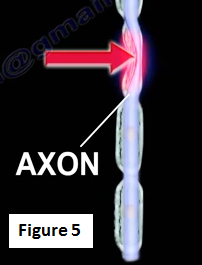
Axonotmesis (Figure 4)
Axonotmesis occurs in crush injuries or displaced bone fractures causing disruption of the nerve cell axon. The axon is damaged while the surrounding connective tissue remains intact (Figure 5). There will be partial or complete recovery of the nerve and Wallerian degeneration occurs distal to the injury site. Recovery depends on the regrowth of the axon and also the distance that is involved. Recovery occurs 1 mm per day or 1 inch per month. There will be fibrillation and positive sharp waves on the EMG study. With re-innervation and recovery, the motor unit potentials will be seen. No conduction velocity distal to the lesion and axonal sprouting and regeneration usually occurs. Recovery is possible without surgery and it may take several months.

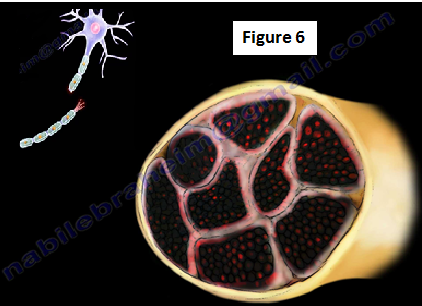
Neurotmesis (Figure 6)
Neurotmesis occurs with knife lacerations, gunshot wounds or severe ischemic injuries. The axon and surrounding connective tissues are damaged, this is the most serious nerve injury. No recovery will take place, fibrillation is present and surgery is usually required. The motor neuron unit potential is usually absent. If the motor unit potential is found, it means the axon has been spared.
An example of a lacerated nerve is a slashed wrist. A penetrating cut at the wrist that affects the flexor carpi radialis tendon will most likely injure the median nerve (Figure 7).

Neurapraxia may be associated with brachial plexus injuries such as "stinger" or "burner" injury, commonly seen in football players. This injury usually improves (Figure 8).

Neurapraxia of the radial nerve, or "Saturday Night Palsy", occurs from compression of the radial nerve at the spiral groove of the humerus (Figure 9).

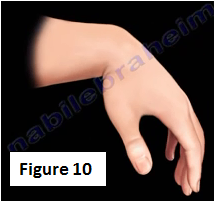
Radial nerve palsy associated with a humerus fracture could show signs of neurapraxia with wrist drop, which later recovers. The patient is observed and the physician will usually obtain an EMG at 6 weeks. However, open fractures of the humerus with radial nerve palsy may have an associated nerve laceration (type III neurotmesis nerve injuries). In this situation, the radial nerve should be explored and the laceration should be repaired. Because of injury to the radial nerve, the patient may experience the condition known as "wrist drop" and the patient may benefit from a wrist splint (Figure 10).
Peripheral nerves have the ability to regenerate. The muscle fiber (axon) is very long, it travels a long distance towards its target (muscle). A long time is needed for the peripheral nerve to recover so it can reach its target and achieve good function.
For more on nerve injuries, follow the links below:
https://www.youtube.com/watch?v=kSeXPm_CFmc
https://www.youtube.com/watch?v=cuRZzUpEW_8
https://www.youtube.com/watch?v=XAwTj9ke4J8
https://www.youtube.com/watch?v=iHBX9NscA40
https://www.youtube.com/watch?v=XQmdeVUUrYw
https://www.youtube.com/watch?v=MeQ12Vi-zt0
https://www.youtube.com/watch?v=Vv78MFi-HRY
For more information on various topics, visit my YouTube Channel:
https://www.youtube.com/user/nabilebraheim