Rotator cuff tears are a common source of shoulder pain. A tear of the rotator cuff may involve a single tendon or multiple cuff tendons (Figure 1).

The patient will present with a painful, weak shoulder (Figure 2). It occurs more in the older population. In patients older than 80 years of age, 50% of these patients will have rotator cuff tear (majority are asymptomatic). Partial thickness or full thickness tears may progress in size or increase in symptoms.

Evaluation
When examining the patient, the physician will find that when a patient is younger than 40 years old with a history of trauma, or a patient who is older than 60 years, without a history of trauma are likely to have the rotator cuff tears. When the patient is between 40-60 years of age there can be either trauma or no trauma.
Clinical Presentation
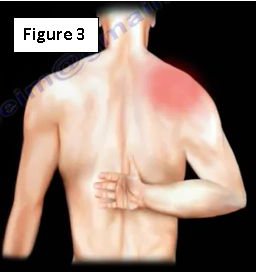
The patient will have pain or aches usually posteriorly. The pain can be in the arm or shoulder. The patient will complain of pain during overhead activity or when attempting to reach behind the back (Figure 3). The patient may also complain about the presence of nighttime shoulder pain. Night pain means that non-operative treatment will not work. The patient may also have shoulder weakness. Rotator cuff tears may be found in patients with a spinal cord injury, due to overuse syndrome.
Rotator Cuff Examination
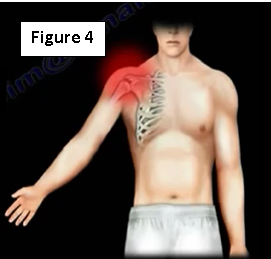
Inspect the shoulder area first! Infraspinatus muscle atrophy may be present and may be a sign of a chronic rotator cuff tear. It may also be a sign of injury to the suprascapular nerve. The physician will palpate the AC joint, as it often has an AC joint pathology. Also check the greater tuberosity of the humerus, the coracoid process and the long head of the biceps tendon. Active and passive range of motion will also be performed. Range of motion may be limited (Figure 4)!
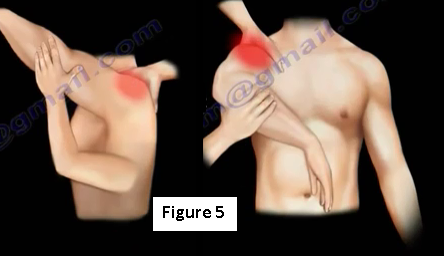
The Neer test and the Hawkin's impingement sign will be performed (Figure 5). Following those tests, strength testing will be conducted. The patient will have weakness of abduction, which tests the supraspinatus function. The physician will also test the external rotation of the arm against resistance, which tests the infraspinatus function. The horn blower's sign will test for a massive tear or a tear of the teres minor muscle. The drop arm test will also be used to test the function of the supraspinatus.
For the subscapularis, there will be three majors test performed. The lift-off test will be used to assess the upper subscapularis muscle (important part) (Figure 6). The patient will be unable to hold the hand behind their back. The belly press test is used to assess the lower subscapularis muscle. It is sometimes called the "abdominal compression test". The third test is the excessive passive external rotation. If the subscapularis tendon is ruptured, it will move medially and the long head of the biceps tendon will sublux with the ruptured tendon.

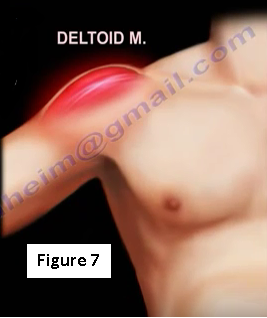
The deltoid strength will also need to be checked to make sure there is a functional deltoid muscle (Figure 7).
A small tear size is up to 1 cm. A medium tear size will measure 1-3 cm. A large tear size will measure 3-5 cm. A massive rotator cuff tear will measure greater than 5 cm, or involve multiple tendons (Figure 8).

Imaging
Once the clinical diagnosis is established, get x-rays! Get true AP view x-rays and check the acromiohumeral interval (normally between 7-14 mm). Get an MRI! T2 images are the best for showing the tear. The sagittal view MRI will help to view the fatty infiltration, muscle atrophy and the retraction of the muscle. This will help to identify if the case is chronic or acute. Using a dye with MRI will also help in seeing partial thickness rotator cuff tears (Figure 9).
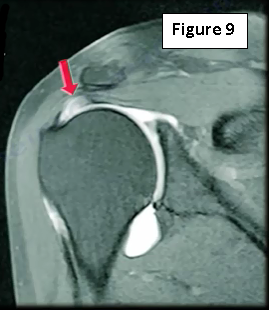
If the patient has a pacemaker, the physician will use CT arthrography instead of an MRI. Some physicians will prefer to use ultrasounds. Remember, an MRI will have a lot of false positives, especially in the elderly population.
Treatment
Treatment will begin conservatively with physical therapy, NSAIDs and injections (possibly). Surgery is usually done when there is a traumatic tear. It will also be done when there is a failure of conservative treatment.
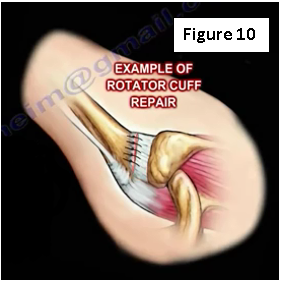
Complete tears of the rotator cuff will not heal on their own! A complete tear of the rotator cuff tendon will need to be sutured back to its insertion into the humeral head (Figure 10). When the rotator cuff tear is large or the patient is older, the prognosis for successful repair is not as good! Muscle atrophy and fatty infiltration will also cause a poor prognosis.
For more information on rotator cuff injuries, follow the links below:
https://www.youtube.com/watch?v=H91veR0dRfY
https://www.youtube.com/watch?v=k_D6KBId740
https://www.youtube.com/watch?v=BwDbo3IqFZU
https://www.youtube.com/watch?v=xn-c2goYzLE
https://www.youtube.com/watch?v=CuZPBxaw5yc
https://www.youtube.com/watch?v=kmNousfSntY
https://www.youtube.com/watch?v=twWWa7F5qxU
https://www.youtube.com/watch?v=1m08kWgo5dc
For more information, visit my YouTube Channel:
https://www.youtube.com/user/nabilebraheim