
The need for entitlement reform should be obvious to anyone. Social Security will slash retiree benefits in two decades without a course correction, Medicare spews red ink and low-value care, and the Affordable Care Act has not produced affordable care. These programs dominate the discussion, and they do need reforms.
But meanwhile, in the past 50 years, Medicaid has transformed from a targeted program for the neediest to the largest health program in the country. It covers more than 70 million individuals -- over 20 percent of our nation's population -- and faces challenges in mission-focus, quality and conforming to current budget realities.
Medicaid consumes ever-larger fractions of federal and state budgets. Federal Medicaid spending increased 13 percent between 2013-14 and 14 percent between 2014-15. It accounts for more than 9 percent of the federal budget and nearly a quarter of states' budgets, in part because Medicaid spending per beneficiary is 1.4 times greater than spending per privately insured individual, despite lower reimbursement rates.
It spends these taxpayer dollars, but produces low-quality care and recent studies have found that many Medicaid recipients have trouble accessing ordinary care. In California, increased emergency room visits are directly correlated with expansion in Medicaid eligibility from 2013 to 2014. Even imposing cost-sharing for inappropriate use of the emergency room has not led to a decline in use by Medicaid recipients, which may indicate that these individuals have no other choice but to seek care in the emergency room.
Conservative policy analysts have proposed block grants (large lump sum payments determined by a formula), capped allotments (basis for funding in the successful Children's Health Insurance Program), and per capita allotments (a fixed amount of funding per enrollee) as ways of dealing with the fiscal distress. However, simply providing less money does not actually reduce the costs of health care; rather, it reduces expenditures without any guarantee of the quality of services or access to them. Underneath these fiscal reforms must be delivery system reforms that generate more efficient and effective medical care.
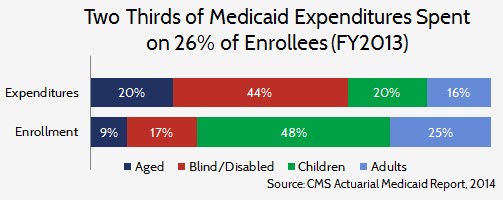
This is a challenge. Medicaid serves a quite heterogeneous population, with a disproportionate amount of spending focused on the blind and disabled. (See the chart below.) More generally, the costs per enrollee differ markedly across the categories of enrollees and reforms will have to be tailored to each group.
It is time to reform entitlement programs. In doing so, Medicaid must not be forgotten. It is the nation's largest health program, faces a daunting financial outlook and delivers low-quality care -- when it delivers care at all. It should be reformed to deliver quality care to the neediest Americans and, thus, meet the original intent Medicaid.