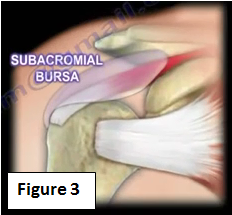
Shoulder impingement syndrome is a common source of pain in the shoulder. It is found in about 50% of patients who come to the doctor with a complaint of shoulder problems. Shoulder impingement is often referred to as rotator cuff tendonitis or shoulder bursitis (Figure 2). It is really an irritation of the rotator cuff and could lead to break down and tear of the tendon. It could be considered an overuse syndrome (Figure 3).
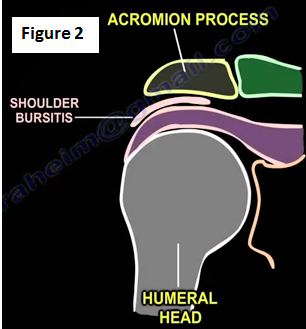
The subacromial bursa is located above the tendon of the supraspinatus rotator cuff muscle (Figure 3). The acromion process of the scapula is above the subacromial bursa. As you lift the arm up, the rotator cuff tendons may become easily irritated because there is bone both above and below these tendons. When the tendons become squeezed and irritated, it causes pain.
How do you diagnose it?
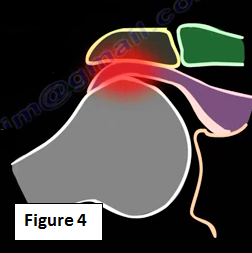
The doctor will start with the patient's history; pain in the shoulder will be increased with overhead activity (Figure 4). If the patient has night pain, it is probably a rotator cuff tear and nonoperative treatment will not work.
Examination
When testing the shoulder for possible impingement, be sure to warn the patient before beginning the examination because this may cause pain in the shoulder (Figure 5).
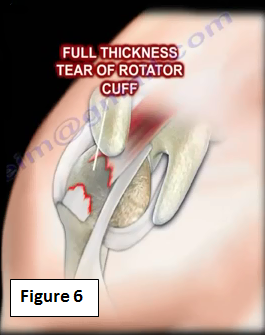
The idea of this impingement test is that the humeral head will squeeze the rotator cuff tendons are possible cause pain. The presence of this continued irritation could lead to a full thickness tear of the rotator cuff tendon (Figure 6).
Neer Impingement Sign
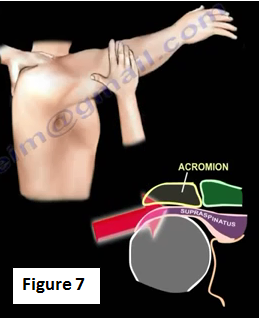
Pinching of the rotator cuff tendon by the underside of the acromion. The examiner stabilizes the scapula with one hand and then moves the arm up in forward flexion attempting to pinch the rotator cuff against the acromion (Figure 7). A pain response due to the impingement is considered to be a positive sign.
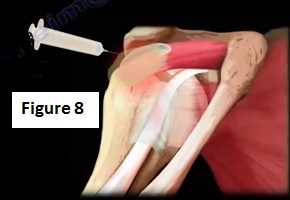
The diagnosis is confirmed when the pain symptoms are relieved by injection of numbing medicine in the subacromial space (10 mL of 1% Xylocaine). The doctor may add 2 cc of corticosteroids to the numbing medicine (Figure 8). When the pain symptoms are relieved and the patient feels better due to the injection.
Hawkin's Sign
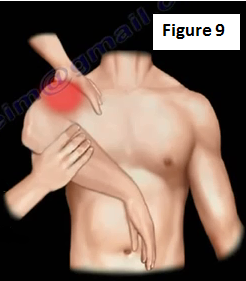
Flex the shoulder to 90° and flex the elbow to 90° as well (Figure 9). Internally rotate the shoulder, which brings the greater tuberosity of the humerus underneath the acromion, which could cause impingement and pain. Pain caused by this impingement is considered to be a positive Hawkin's Sign.
Imaging
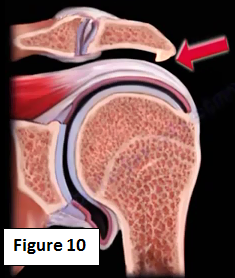
X-rays can show the bone spur of the acromion which is a prominence on the under surface of the acromion. The bony acromial spur digs into the tendon of the rotator cuff (Figure 10).
A true anteroposterior view x-ray should be obtained; the patient can be standing, sitting or lying down (Figure 11). This view will show the acromiohumeral interval, which is normally about 7-14 mm.

A scapular Y view lateral x-ray will show the bony acromial spur and what type of acromion is present (Figure 12).

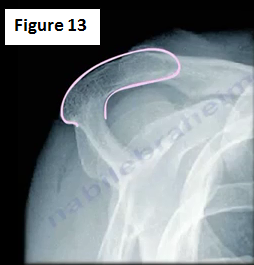
The supraspinatus outlet view x-ray will show the acromion morphology (Figure 13). Type III Hooked acromion is most often associated with rotator cuff pathology.
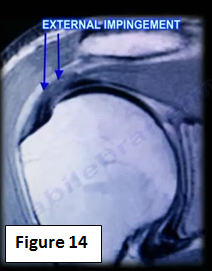
An MRI study is helpful in displaying the associated rotator cuff pathology (Figure 14).
Treatment
The initial treatment is nonoperative and includes NSAIDs (nonsteroidal anti-inflammatory drugs), like Motrin. This medication may have side effects. Always ask the doctor about any potential side effects. Physical therapy will also be utilized for the front and back shoulder muscles. This will give the shoulder more room to move. Physical therapy will be an aggressive cuff strengthening and periscapular muscle stabilization exercises. The aim is to coordinate the muscles and to regain full range of motion of the shoulder (Figure 15).

Treatment can also commonly be a subacromial injection of numbing medicine and steroids (Figure 16). The injection is used in hopes of decreasing the level of inflammation. If the patient improves, then we have the correct diagnosis. Some physicians use blind injection technique (I will use the blind technique initially).

With additional injections, I will use the ultrasound guided injection technique. The injection is into the subacromial bursa and not the tendon. I then will ask the patient to come back in six weeks. During this follow-up appointment, I will repeat the injection. At this point, if the patient is not improving, an MRI will be ordered and we will dig deeper. The MRI will give us a better idea of any other pathology that may exist. We need to rule of the possibility of a rotator cuff tear. If the result is that the patient has impingement of the shoulder that is not improving and there is significant pain despite conservative treatment, then we will need to perform surgery. The surgery will be performed after conservative treatment has failed for about 4-6 months. Studies show that the surgical outcome is usually not as good in patients with workers' compensation claims.
Subacromial Decompression
We will shave the under surface of the acromion in order to create more room for the rotator cuff tendon. Removal of the subacromial bursa and bone on the underside of the acromion is performed. If there is pain from the AC joint associated with impingement, then the surgeon will probably need to excise the outer portion of the clavicle. The biceps tendon is connected to the rotator cuff associated tendonitisis. The physician may need to perform a biceps tendon tenotomy or biceps tenodesis. The result of surgery is usually very good if the doctor has the proper patient, proper clinical situation, proper diagnosis and a positive injection test.
After surgery, the patient will be given a sling for a few days. The patient will return to normal daily activity within a couple weeks. At two weeks, the patient will be able to lift the arm above the head. At two months, the patient's will have a near normal condition.
Complications
Complications after surgery may occur and usually involve deltoid muscle disruption. The doctor will do either an acromionectomy (excise a large portion of the acromion) or excision of the Os Acromial, which will lead to deltoid muscle dysfunction. They may need the Os Acromiale to heal first and then later do the acromioplasty. The Os Acromiale is seen in an axillary view.
Excision of the CA ligament in a patient with a massive rotator cuff tear. In these types of patient, the doctor should try to avoid a coracoacromial ligament release to present the coracoacromial ligament.